
Everything You Need to Know About Medicare’s New GLP-1 Coverage
Starting July 1, 2026, Medicare GLP-1 coverage opens up for the first time. Eligible patients can get Wegovy (semaglutide), Zepbound (tirzepatide), or Foundayo (orforglipron) for a $50 copay through December 31, 2027. The program is called the Medicare GLP-1 Bridge, and for the right patient it is the best deal on the market right now.
It is also smaller than the headlines make it sound, and there are three things the celebration coverage skipped. I want to walk through who qualifies, what it actually costs, and the catches you need to understand before you assume this fixes your access problem.
What the Medicare GLP-1 Bridge actually is
The Bridge is a CMS demonstration program, not a permanent change to Part D. CMS announced it in December 2025 as a short-term bridge to a longer-term program called BALANCE.1 The original plan was a six-month pilot through the end of 2026, after which BALANCE would take over and shift the cost from the federal government to the Part D plans.
That handoff did not happen. When the April 20, 2026 deadline came for insurance plans to opt into BALANCE for 2027, not enough of them signed up to meet the participation threshold. CMS pulled the plug on the Medicare side of BALANCE and extended the Bridge through December 31, 2027 instead.2 So instead of a six-month pilot, we now have an 18-month program with no confirmed replacement after it ends.
Here is what makes the Bridge unusual. It does not run through your Part D plan. CMS contracts Humana as a central processor, and the prior authorization and claims go directly to that processor. Your Part D plan does not have to opt in, does not bear any of the cost, and does not need to do anything for you to use the program. If you are enrolled in any standalone Part D plan or a Medicare Advantage plan with drug coverage, and you meet the clinical criteria, you can use the Bridge.
Who qualifies for the Medicare GLP-1 Bridge
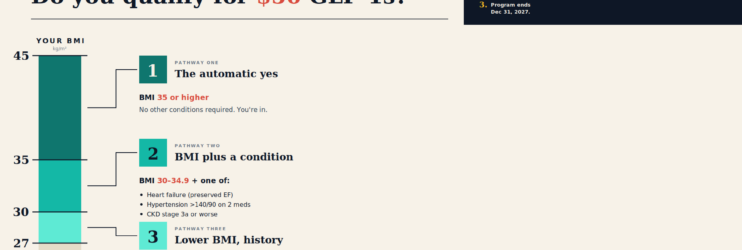
There are three pathways. You only need to meet one. The BMI used is your BMI at the time you first started GLP-1 therapy, not your current BMI. If you started a GLP-1 a year ago with a BMI of 38 and you are now down to 33, your prescriber attests to the higher number and you still qualify.

The criteria come straight from the CMS prior authorization rules.3 The full list:
| Pathway | BMI at start of GLP-1 therapy | Qualifying condition needed? |
|---|---|---|
| 1 | 35 or higher | None. The BMI alone qualifies you. |
| 2 | 30 to 34.9 | Heart failure with preserved ejection fraction, uncontrolled hypertension (above 140/90 on two meds), or chronic kidney disease stage 3a or worse. |
| 3 | 27 to 29.9 | Pre-diabetes (ADA criteria), prior heart attack, prior stroke, or symptomatic peripheral artery disease. |
A few things worth noticing. Pathway 2 specifies uncontrolled hypertension. Garden-variety high blood pressure that is well-controlled on a single medication does not qualify. The bar is blood pressure still above 140/90 despite two antihypertensives. Pathway 3 includes pre-diabetes, which by ADA criteria means a fasting glucose of 100 to 125, an A1c of 5.7 to 6.4, or a two-hour glucose tolerance of 140 to 199. If your A1c has been creeping up over the last few years and you are in that range, you probably qualify.
What drugs the Medicare GLP-1 Bridge covers
Three medications, with one wrinkle on Zepbound.
| Drug | Formulations covered | Manufacturer |
|---|---|---|
| Wegovy (semaglutide) | All injectable doses and oral Wegovy tablets. | Novo Nordisk |
| Zepbound (tirzepatide) | KwikPen only. Single-dose vials and single-dose pens are not covered. | Eli Lilly |
| Foundayo (orforglipron) | All formulations of the recently approved oral GLP-1. | Eli Lilly |
The Zepbound situation is worth a second look. Only the KwikPen formulation is included. The single-dose vials and single-dose pens are not. If your prescriber writes for vials, the claim will be rejected. You have to switch to the KwikPen to use the Bridge.
Ozempic and Mounjaro are not on the Bridge list at all, because both are FDA-approved for diabetes rather than for weight management. If you are on either of those for diabetes, you keep getting them through your regular Part D plan.
When Medicare GLP-1 coverage applies outside the Bridge Program
This is the part most patients do not realize. Medicare has been covering GLP-1s for years, just not for weight loss. By federal law, Part D cannot cover any drug used solely for weight management. But when the same drug is prescribed for an FDA-approved indication other than obesity, standard Part D coverage applies, and the medication counts toward your deductible and your $2,100 out-of-pocket cap.
Here is the current map of what Part D will cover when a GLP-1 is prescribed for something other than weight loss:
| Drug | Covered indication under standard Part D | Coverage notes |
|---|---|---|
| Ozempic (semaglutide) | Type 2 diabetes. Also: CV risk reduction in T2DM with established heart disease, and kidney disease in T2DM. | Widely covered on Part D formularies. Prior auth and step therapy common. |
| Mounjaro (tirzepatide) | Type 2 diabetes. | Covered by most Part D plans. Often requires step therapy through metformin first. |
| Rybelsus (oral semaglutide) | Type 2 diabetes. | The oral diabetes formulation. Not the same as oral Wegovy. |
| Trulicity (dulaglutide), Victoza (liraglutide) | Type 2 diabetes. | Older GLP-1s. Often the cheapest covered option but less potent. |
| Wegovy (semaglutide) | CV risk reduction in adults with established cardiovascular disease and BMI 27 or higher. Also: MASH with stage F2 to F3 liver fibrosis (no cirrhosis). | MASH was added in 2025. Coverage depends on documentation of the qualifying condition. |
| Zepbound (tirzepatide) | Moderate-to-severe obstructive sleep apnea in adults with obesity. | Sleep study documenting OSA is typically required for prior auth. |
A few things to understand about this table.
For type 2 diabetes, almost any Part D plan covers at least one GLP-1, though specific formulary choices vary by plan. Step therapy is the norm: most plans want documentation that you have tried metformin first. Once you are on a GLP-1 for diabetes, your plan covers it indefinitely as long as you remain on the medication for that indication.
For Wegovy’s cardiovascular indication, you need documented established cardiovascular disease, meaning a prior heart attack, stroke, or known coronary artery disease, plus a BMI of 27 or higher. This was approved by the FDA in 2024 and Medicare followed. If you have had a cardiac event and you are also overweight, this is often a better coverage path than the Bridge because the drug cost counts toward your annual out-of-pocket cap.
For Wegovy’s MASH indication, you need a liver biopsy or non-invasive testing documenting stage F2 or F3 fibrosis with metabolic-associated steatohepatitis. This indication was added in 2025 and is still working its way into Part D formularies. Coverage criteria vary by plan, and some plans are still requiring the cardiovascular criteria as a stand-in until they update their formulary language.
For Zepbound’s sleep apnea indication, you need a sleep study documenting moderate-to-severe obstructive sleep apnea (apnea-hypopnea index of 15 or higher) plus obesity. Approved in late 2024. Like the Wegovy CV indication, this is often the better path than the Bridge if you qualify clinically, because the drug counts toward your cap.
One important wrinkle: if a GLP-1 is coverable under standard Part D for one of these indications, it cannot be obtained through the Bridge for weight management.4 The Bridge is specifically a weight-management-only program. The federal rule is that you cannot use the Bridge to access a drug that your Part D plan would cover for another indication. If you have type 2 diabetes and you want Ozempic, you go through Part D. If you have established heart disease and you want Wegovy, you go through Part D. The Bridge fills the gap where weight management alone is the medical reason for the prescription.
This actually matters. A patient with type 2 diabetes, hypertension, and obesity who qualifies for a GLP-1 under multiple indications should usually take the Part D diabetes coverage over the Bridge. Same drug, but the diabetes route counts toward the $2,100 cap. The Bridge does not.
The three catches with the Medicare GLP-1 Bridge
This is where the celebration coverage stops and the real story starts.
Catch 1: The $50 does not count toward your Part D cap
Medicare Part D has an annual out-of-pocket cap. Once you hit $2,100 in 2026 ($2,400 in 2027), the rest of your covered drugs that year are free. That is one of the most important pieces of senior drug protection on the books.
The Bridge copay does not count toward that cap.5 The $50 you pay every month for your Wegovy or Zepbound is on top of whatever you are spending to hit your cap. It does not count toward your deductible either. Twelve months of Bridge copays adds $600 a year that is completely outside your normal Part D protection.
If you are managing five chronic conditions and you are used to your medications going free once you cross the cap each year, this changes the math. The GLP-1 is the one drug that keeps charging you every month, no matter what.
Catch 2: Extra Help does nothing here
Medicare Extra Help, also called the Low-Income Subsidy, is a federal program that drops drug copays for low-income seniors. If you qualify for Extra Help, your normal Part D copays are around $5 for generics and $10 for brand-name drugs.
Extra Help does not apply to the Bridge.6 If you are on Extra Help and you want a GLP-1 for weight loss, you pay the same $50 a month as anyone else. The seniors who can least afford it go from $5 to $50 for one prescription, while their other medications stay subsidized.
This is the part that bothers me most about how the program is structured. The framing in the press releases is that this opens GLP-1s to Medicare patients. In practice, it opens them to Medicare patients who can find $600 a year of disposable income that does not go toward anything else they need. That is not nothing, but it is not the universal access the headlines suggest.
Catch 3: The Bridge ends December 31, 2027, with no confirmed replacement
BALANCE was supposed to be the long-term answer. The structure was straightforward: CMS would negotiate prices with the manufacturers, and Part D plans would voluntarily opt in to a program with standardized coverage rules for GLP-1s for obesity. Patients in participating plans would pay something like the current Bridge copay, but the cost would shift from the federal government to the insurer.
Not enough plans signed on. CMS confirmed in April 2026 that the participation threshold for BALANCE in Medicare Part D was not met for 2027.7 On UnitedHealth’s earnings call that same week, the CEO of their government programs division said the company was still working through “notable challenges and outstanding questions with the currently planned structure.” Translation: covering GLP-1s for obesity adds billions to plan costs, and the financial incentives in the model were not enough to make it worth their while.
So the Bridge runs through the end of 2027, CMS is collecting utilization data to share with plans, and at some point in 2027 there will be another opportunity for plans to opt into BALANCE for 2028. They might. They might not. Right now, no one knows what happens to your $50 GLP-1 after January 1, 2028.
A few scenarios. Enough plans sign on for 2028, BALANCE launches, and you keep your coverage at something close to current cost. Not enough plans sign on, CMS extends the Bridge again, and you keep the $50 deal. Or neither happens, the Bridge expires, BALANCE never launches in Part D, and Medicare patients on GLP-1s for weight loss have no coverage at all. The third scenario is the one nobody talks about, and right now it is on the table.
Timeline at a glance
- December 2025: CMS announces the Bridge and the BALANCE Model.
- April 20, 2026: Deadline for Part D plans to opt into BALANCE for 2027. Threshold not met.
- April 21, 2026: CMS announces BALANCE will not launch in Medicare Part D in 2027 and extends the Bridge through end of 2027.
- July 1, 2026: Bridge goes live. Prior authorizations open through Humana as the central processor.
- December 31, 2027: Bridge expires.
- January 1, 2028: BALANCE may launch if enough plans opt in for the 2028 plan year. May not.
What to do if you think you qualify
Start the conversation with your doctor in June. The prior authorization process opens July 1, and the central processor is Humana, not your Part D plan. Your prescriber submits the PA directly to the Bridge processor, attests that you meet one of the three pathways, and includes documentation of structured lifestyle modification including nutrition and physical activity guidance consistent with the FDA label.
For your prescriber’s reference, the pharmacy claims route through a dedicated BIN and PCN specific to the Bridge.8 If you fill the prescription at a participating pharmacy and the system is set up correctly, you pay $50 and walk out.
A few practical points. Doctors do not need to be enrolled as Medicare providers to write the prescription or submit the prior authorization, so a telehealth physician who is not in the Medicare network can still help you access the Bridge. If you have been on a GLP-1 for years and have lost weight, your prescriber attests to your BMI at the time you started therapy, not your current BMI. And if your current prescriber is writing for Zepbound vials, ask whether the KwikPen is appropriate before July 1 to avoid a coverage gap.
When the Bridge is actually the wrong move
Two situations where I would think twice before signing up.
If you qualify for any of the standard Part D indications above (diabetes, established cardiovascular disease, MASH, or sleep apnea), use Part D instead. The plan copay may be higher than $50, but the drug counts toward your deductible and your $2,100 cap. For patients with significant other prescription costs, that protection matters more than the per-fill price.
If you are on Extra Help and the $50 is competing with other essential medications, that is a real conversation to have with your prescriber. The right answer is not always the GLP-1. There are lower-cost weight loss approaches that may make more sense given your full budget.
Bottom line on Medicare GLP-1 coverage
If you qualify, you have a Part D plan, the $50 is manageable on top of your other drug spending, and you are not on Extra Help, the Bridge is the best deal on the market for Medicare-eligible patients right now. Talk to your doctor in June. Get the prior authorization in the queue early. Switch to a Zepbound KwikPen if you are on vials.
But read the fine print first. For a meaningful number of Medicare patients, especially the ones the program was supposed to help most, the Bridge is not the deal the press releases make it sound like. Know what you are signing up for before you sign up.
Want a doctor who has already read the fine print?
Sign up for the Barrick Health Insider newsletter for ongoing coverage of the Bridge, BALANCE updates as they come, and the clinical detail that does not make it into the press releases.
If you want a one-on-one read on your situation, book a free consultation with me.
Clete
References
- Centers for Medicare & Medicaid Services. “Medicare GLP-1 Bridge.” Updated April 2026. cms.gov/medicare/coverage/prescription-drug-coverage/medicare-glp-1-bridge
- Kaiser Family Foundation. “What to Know About the BALANCE Model for GLP-1s in Medicare and Medicaid and the Medicare GLP-1 Bridge.” Updated May 11, 2026.
- CMS Medicare GLP-1 Bridge FAQs, Eligibility Criteria, March 2026. The BMI used is the BMI at the time the patient first started GLP-1 therapy, not their current BMI.
- CMS Medicare GLP-1 Bridge FAQs. Beneficiaries prescribed an eligible GLP-1 for a use coverable under standard Part D (e.g., Wegovy for CV risk reduction, Zepbound for OSA) do not qualify for that drug under the Bridge. CMS monitors Part D formulary practices to prevent plans from shifting coverage to the Bridge.
- CMS Medicare GLP-1 Bridge FAQs. The $50 copay does not count toward the Part D deductible or the annual out-of-pocket maximum ($2,100 in 2026, $2,400 in 2027).
- CMS Medicare GLP-1 Bridge FAQs. “For beneficiaries enrolled in the Low-Income Subsidy (LIS) program, the LIS cost-sharing subsidies will not apply in the Medicare GLP-1 Bridge.”
- Fierce Healthcare. “CMS delays Part D GLP-1 model amid skepticism from insurers.” April 21, 2026.
- Pharmacy BIN 028918, PCN MEDDGLP1BR. Humana administers the central processor for the Bridge on behalf of CMS.
This content is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before starting, stopping, or changing any medication or treatment. If you would like personalized guidance, you can book a free consultation with Dr. Barrick.