
GLP-1 Hair Loss: What’s Actually Happening (and What to Do About It)
GLP-1 Hair Loss: What’s Actually Happening (and What to Do About It)
By Dr. Clete Barrick, MD
Board-Certified Internal Medicine & Obesity Medicine | Barrick Health
GLP-1 hair loss is almost always telogen effluvium, a temporary shedding triggered by rapid weight loss, not by the medication itself. Over 95% of cases resolve on their own once your weight stabilizes and your nutrition improves. The single most important thing you can do about it? Fix your protein intake. That one change matters more than every supplement on the shelf combined.
What Is Telogen Effluvium (and Why Your Shower Drain Looks Like a Crime Scene)
Your hair grows in cycles. There’s a growth phase (anagen), a short transition phase (catagen), a resting phase (telogen), and then the follicle sheds and starts over. Under normal conditions, about 10% of your hair sits in the resting phase at any given time. You lose 50 to 100 hairs a day and never notice.
When your body goes through significant metabolic stress (rapid weight loss qualifies), it pushes a much larger percentage of follicles into the resting phase all at once. Instead of 10%, you might have 30 to 50% of your follicles parked in telogen simultaneously. Two to four months later, they all shed together.
Here’s the part that confuses almost everyone: the timing. You started the medication in January. The shedding starts in April. You blame the drug. But those follicles made the decision to rest months ago, during the period of rapid caloric deficit and metabolic change. The trigger was the stress of fast weight loss, not the molecule sitting in the syringe.
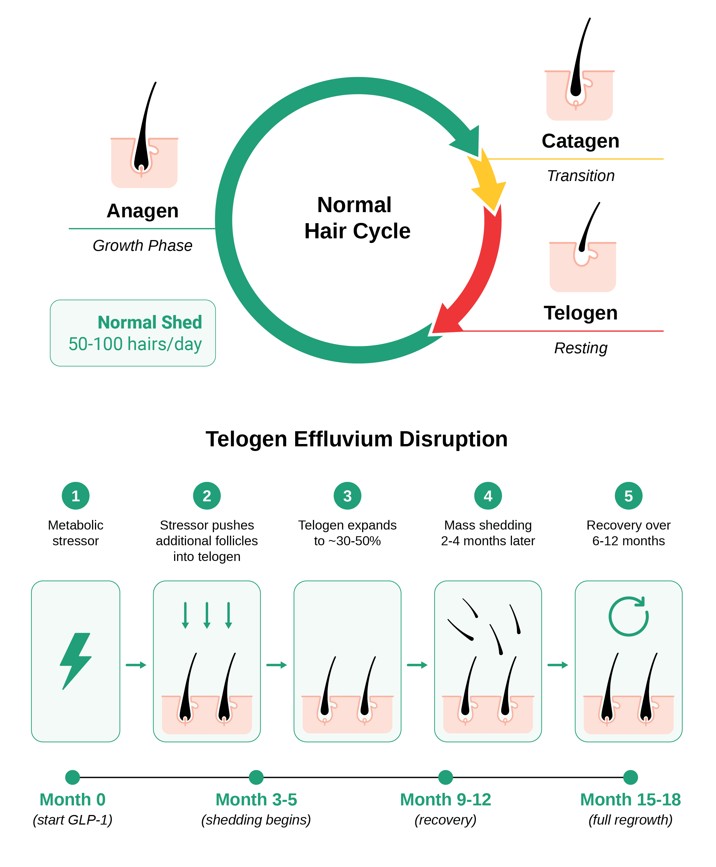
Hair Growth Cycle and Telogen Effluvium. From The GLP-1 Bible by Dr. Clete Barrick. The bottom timeline shows the typical course for GLP-1 patients: shedding begins around months 3 to 5, recovery starts by months 9 to 12, and full regrowth is expected by months 15 to 18.
How Common Is This, Really?
The Wegovy clinical trials reported alopecia in 3% of the treatment group versus 1% on placebo.1 But that headline number hides the real pattern. When researchers broke it down by how much weight patients lost, the picture got sharper: 5.3% of patients who lost more than 20% of their body weight experienced hair loss, compared to just 2.5% of those who lost less than 20%.1 The faster you lose, the more you shed.
A systematic review published in April 2026 analyzed 24 studies on GLP-1 medications and hair loss.2 Semaglutide and tirzepatide carried the highest incidence among GLP-1 drugs, with tirzepatide (the one that produces the most weight loss) most frequently linked to telogen effluvium. The effect appears dose-dependent for semaglutide: doses under 2 mg per week were rarely associated with hair loss, while higher obesity-treatment doses showed up more often. Women were disproportionately affected.
A separate real-world study of nearly 550,000 patients found increased odds of both telogen effluvium and androgenetic alopecia at 12 months in GLP-1 users, independent of age, sex, BMI, and diabetes status.3 FDA adverse event data tells a similar story: semaglutide carried a reporting odds ratio of 2.46 for alopecia, tirzepatide 1.73.4
So yes, this is a real and common side effect. But “common” and “permanent” are very different words.
The Good News: It Comes Back
Over 95% of the time, GLP-1 hair loss is self-limiting. Once your weight stabilizes and your nutrition improves, the follicles cycle back to the growth phase on their own. The typical timeline is 6 to 12 months after the shedding starts, which puts full regrowth at roughly 15 to 18 months from when you began the medication (see the timeline in Figure 25.2 above).
I had a patient text me a photo of her shower drain at 11 PM, convinced the medication was poisoning her. Her hair had made that decision three months before she ever filled the prescription. Three months later, she could already see the regrowth coming in.
The same principle that protects your muscle protects your hair: lose at a controlled pace. I call it the Golden Rule. Half a pound to 3 pounds per week. If you’re losing faster than that, your body is under more metabolic stress than it needs to be, and your hair is one of the first places that stress shows up.
The First Thing I Check: Protein
This is the part most people skip. And it’s the single most important variable I investigate when a patient tells me their hair is falling out.
When you’re not getting enough protein for your body’s needs, your body starts making business decisions with the limited supply it has. Skeletal muscle, heart, brain, liver, kidneys: those are required for survival. Hair is not. Hair follicles are the first to get furloughed.
Think of your hair as a canary in the coal mine for protein status. When the canary goes quiet, it’s telling you something about the air quality. You can take every supplement on the shelf. You can rub minoxidil on your scalp twice a day. But until you fix the protein deficit, you’re treating a symptom while ignoring the cause.
⊕ Dr. Barrick’s Protein Prescription: Add a minimum of 30 grams of protein per day above wherever you are right now. Whey shakes, Greek yogurt, eggs, cottage cheese, whatever gets you there. Don’t wait for labs. Don’t wait for a dermatology referral. Start today.
GLP-1 medications suppress appetite. That’s the whole point. But reduced appetite means reduced food intake, and reduced food intake means most patients aren’t hitting adequate protein targets unless they’re actively tracking it. This is fixable. But you have to be intentional about it.
The Lab Panel That Actually Matters
After protein, get these checked:
| Lab | Target | Why It Matters |
|---|---|---|
| Ferritin | >40 ng/mL | Most lab reports flag anything above 12 as normal. Dermatologists specializing in hair loss want it above 40. Big difference. |
| Zinc | Within range | Zinc deficiency impairs hair follicle function. Common in caloric restriction. |
| Vitamin D | >40 ng/mL | Low vitamin D is linked to telogen effluvium. Optimal is 40 to 60, not the 30 most labs call sufficient. |
The one I want to flag specifically: ferritin.8 This is the lab that trips people up. Your doctor runs the panel, sees a ferritin of 15, and tells you it’s normal. Technically, by standard reference ranges, it is. But dermatologists who specialize in hair loss know that hair follicles need ferritin above 40 to function optimally. If you’re at 15 and shedding, that’s not a coincidence.
The Biotin Problem
Biotin is the supplement everyone reaches for. It’s in every hair vitamin on the market. It has a multi-billion-dollar marketing engine behind it. And for GLP-1 hair shedding specifically, the evidence that it helps is essentially nonexistent.
A 2024 systematic review searched the entire published literature for studies on biotin and hair growth.5 They found exactly three studies that met basic inclusion criteria. The highest-quality study (double-blind, placebo-controlled) found no difference between biotin and placebo for hair growth. The other two studied narrow patient populations and had significant methodological problems. That’s the evidence base for a supplement that 40 million Americans take.
But here’s where it gets worse. Biotin doesn’t just fail to help. It can actively cause harm.
⚠ Biotin Warning: High-dose biotin interferes with common laboratory tests. It can produce a falsely normal troponin result (the test used to diagnose heart attacks), false thyroid function results, false cortisol levels, and false hormone panels. The FDA has issued multiple safety communications about this interference, and at least one patient death has been linked to a falsely low troponin result caused by biotin supplementation.6,7
Hair supplements marketed for “hair, skin, and nails” can contain up to 20 mg of biotin per dose. That’s more than 650 times the recommended daily allowance. At those levels, your lab results become unreliable.
As I tell my patients: biotin is a lot better at hiding a heart attack than growing hair. That’s a hard sell on the supplement label, though.
If you’re currently taking biotin, stop it at least 48 to 72 hours before any blood draw.6 For GLP-1 hair shedding specifically? Skip biotin entirely. Fix your protein instead.
Hair Supplements: The Evidence (or Lack of It)
The supplements with the biggest marketing budgets have the smallest evidence base. This pattern repeats across the entire hair supplement industry, and it’s worth understanding how it works.
A company funds a study on its own product. The study finds the product works. No independent researcher replicates the result. The company sells a hundred million dollars of capsules. That’s not science. That’s marketing with a lab coat.
Save your money. Fix your protein.
When Protein and Patience Aren’t Enough
If you’ve addressed your protein intake, corrected any lab deficiencies, and given it six months, but the shedding hasn’t resolved, there are two medications with real evidence behind them.9
| Minoxidil | Finasteride | |
|---|---|---|
| Access | Over the counter (topical or foam) | Prescription only (oral) |
| How it works | Increases blood flow to follicles, extends the growth phase | Blocks DHT, the hormone that shrinks follicles in pattern hair loss |
| Best for | General thinning, telogen effluvium support | Androgenetic (pattern) hair loss specifically |
| Key note | Causes temporary increased shedding (“dread shed”) in the first few weeks. This is the drug working. Do not stop. | Discuss the side effect profile with your physician before starting. Not appropriate for all patients. |
The one thing I want you to hear from me about minoxidil: that initial increase in shedding (the “dread shed”) scares people into quitting. It’s counterintuitive. You start a product to stop hair loss, and in the first few weeks you lose more hair. But the shedding is the medication pushing weak, resting hairs out so that new, stronger growth can replace them. It’s temporary. Don’t stop.
Will My Hair Come Back? (The Question Behind Every Question)
This is what patients actually want to know. The answer depends on what type of hair loss is happening.
| Telogen Effluvium | Androgenetic Alopecia | |
|---|---|---|
| Cause | Metabolic stress (rapid weight loss, caloric deficit, nutritional gaps) | Genetics and hormones (DHT sensitivity) |
| Pattern | Diffuse thinning across the whole scalp | Temples, crown, hairline (male) or widening part (female) |
| Reversible? | Yes. Temporary. Full regrowth expected. | Manageable but progressive without treatment. |
| Timeline | 6 to 12 months to full recovery | Ongoing management required |
| Next step | Fix protein, labs, pace of loss. Patience. | See a dermatologist for diagnosis and treatment plan. |
If this is pure telogen effluvium, the answer is yes. Temporary. Full regrowth.
But rapid weight loss can unmask something that was already developing underneath. Androgenetic alopecia (pattern hair loss) is driven by genetics and hormones. The weight loss didn’t cause it. It revealed it. If your regrowth comes in thinner or finer than before, or the shedding follows a pattern (temples, crown, widening part) rather than diffuse thinning across the whole scalp, that’s a different condition with a different plan. See a dermatologist.
The Hair Loss Hierarchy: Start at the Top, Not the Bottom
If you’re dealing with GLP-1 hair loss, here’s the order. Most people start at the bottom (supplements) and work up. Do the opposite.
| Priority | Intervention | What to Do |
|---|---|---|
| 1 | Protein | Add 30g/day above current intake. Track it. Don’t guess. |
| 2 | Labs | Ferritin >40, zinc, vitamin D >40. Correct any deficiencies. |
| 3 | Patience | 6 to 12 months for natural regrowth. Control your rate of loss (0.5 to 3 lbs/week). |
| 4 | Minoxidil | OTC option if the above haven’t resolved shedding after 6 months. Expect the dread shed. |
| 5 | Supplements | Last resort. Evidence is weak. Skip biotin for GLP-1 shedding. |
Start at the top. Not the bottom.
Going Deeper
Everything I covered here (the protein protocol, the lab targets, the biotin warning, the treatment hierarchy) is one section of one chapter of The GLP-1 Bible. The full book covers the complete picture: dosing strategy, side effect management, nutrition, exercise, long-term planning, and what the research actually says versus what the internet thinks it says. If this post was useful, the book goes ten layers deeper.
Want the Full Protocol?
Join the Barrick Health Insider community (free) for Dr. Barrick’s complete hair preservation protocol, lab interpretation guide, and the specific supplement recommendations he gives patients who have already addressed protein and labs first. Subscribe at barrickhealth.com.
This post is adapted from a Straight Shot episode. Watch the full video for the visual walkthrough, patient stories, and the biotin takedown: [YouTube link]
This content is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before starting, stopping, or changing any medication or treatment. If you would like personalized guidance, you can book a free consultation with Dr. Barrick.
References
1. Novo Nordisk. Wegovy (semaglutide) Prescribing Information. FDA, 2021.
2. Gupta AK, Teasell EM, Economopoulos V, Mirmirani P. GLP-1 therapies and hair loss: A systematic review. Science Progress. 2026;109(2). doi:10.1177/00368504261444578
3. Vidal A, Akiska D, et al. Increased risk of hair loss with GLP-1 receptor agonists: A real-world multicenter TrinetX cohort study. JAAD International. 2026. doi:10.1016/j.jdin.2026.01.014
4. Godfrey H, Leibovit-Reiben Z, Jedlowski P. Alopecia associated with semaglutide and tirzepatide: FAERS disproportionality analysis, 2022-2023. JAAD. 2024.
5. Yelich A, Jenkins H, Holt S, Miller R. Biotin for Hair Loss: Teasing Out the Evidence. J Clin Aesthet Dermatol. 2024;17(8):56-61.
7. Saenger AK, et al. Biotin interference in high-sensitivity cardiac troponin T testing. European Heart Journal. 2022;43(23):2240-2247.
8. Trost LB, Bergfeld WF, Calogeras E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. J Am Acad Dermatol. 2006;54(5):824-844.
9. Branyiczky L, et al. Effects of GLP-1 Receptor Agonists on Hair Loss and Regrowth: A Systematic Review. Int J Dermatol. 2025. doi:10.1111/ijd.70133